‘Doc’, I thought someone had hit me in the leg from behind, but when I looked around, no one was there!’
This is a common presentation for middle-aged ‘weekend warrior’ sports participants. They usually play squash, netball, or touch football and often find it difficult to walk after the injury. It can be quite an explosive event, causing some patients to initially think that they were hit by an opponent with a bat or racquet.
Background
The Achilles tendon is the largest tendon in the body and unusually crosses three joints. Achilles tendon rupture is a common injury that can cause long-term disability if not treated promptly.
Diagnosis is clinical with observation of a tendon gap and a positive calf squeeze test (Thompsons or Simmonds).
Imaging is useful to exclude associate avulsion fractures (X-Ray) or help define the location and size of tendon gap (US or MRI).
Debate exists on whether surgery (open or minimally invasive) is superior to nonoperative management.
A recent study from the New England Journal of Medicine, entitled "Surgical Treatment of Acute Achilles Tendon Rupture," showed that at one year, there were no significant differences in functional outcomes for patients treated with either surgery, minimally invasive surgery, or a nonoperative approach.
Results
526 patients were included in the final analysis and at 12 months there was no significant differences for functional outcomes (strength, function, quality of life) among groups.
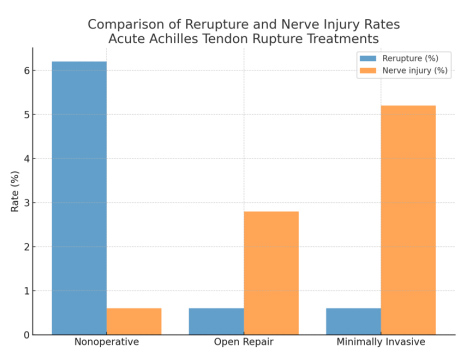
Re-rupture rates though were higher in non-operatively treated patients, whilst nerve injuries were seen more frequently in the minimally invasive group. Perhaps not unsurprising given that the surgeon doesn’t identify the sural nerve during this type of surgery.
Conclusions
For acute Achilles tendon rupture, surgery does not improve one-year functional outcomes compared to nonoperative care, though it reduces re-rupture risk. Treatment choice should balance the slightly higher re-rupture risk of nonoperative care against the surgical risks (nerve injury, wound complications).
A/Prof Higgs’ Preferred Treatment Choice
Given the higher re-rupture rates, it's hard not to recommend surgery for elite athletes. However, for most patients, nonoperative treatment is very reasonable. This is assuming they have had early (within 2 days) treatment with the application of a moon boot, three wedges, and commencement of a functional rehabilitation program. Don’t forget to complete a DVT risk assessment as most will meet the threshold for pharmacological prophylaxis. The size of the gap is intuitively important, but the jury is still out. If an ultrasound shows a gap of greater than two centimetres, I'll usually recommend surgery; if less than two centimetres, I recommend nonsurgical treatment.
I hope you found this update useful, and I'd recommend further reading of the original article. Reference below.
References:
- Myhrvold SB, Brouwer EF, Andresen TK, Rydevik K, Amundsen M, Grün W, et al. Nonoperative or surgical treatment of acute Achilles’ tendon rupture. New England Journal of Medicine. 2022;386(15):1409-20.